
Teen Substance Use: What Parents Need to Know, What It Often Signals, and When to Get Help
Finding out your teenager is using substances is one of the most frightening discoveries a parent can make.
The fear is immediate and total. You think about addiction. About overdose. About futures that narrow before they've had a chance to open. About everything you didn't see, and everything you should have done differently.
And then — once the fear settles enough to think — you face a decision you have almost no framework for making: what do I do with this?
In 30 years of working with families navigating adolescent challenges, this is one of the situations I encounter most often. And the first thing I try to offer is not a plan, but a reframe, because the decisions families make in the first days and weeks after discovering substance use are often shaped by fear in ways that make things harder, not easier.
This guide is my attempt to give parents a clearer, more grounded picture of what teen substance use actually means, what it's usually trying to do, and how to think about the response.
The substance is almost never the whole story. Before you can respond effectively, you need to understand what it's treating — because that's where the real work begins.
First: a reframe that changes everything
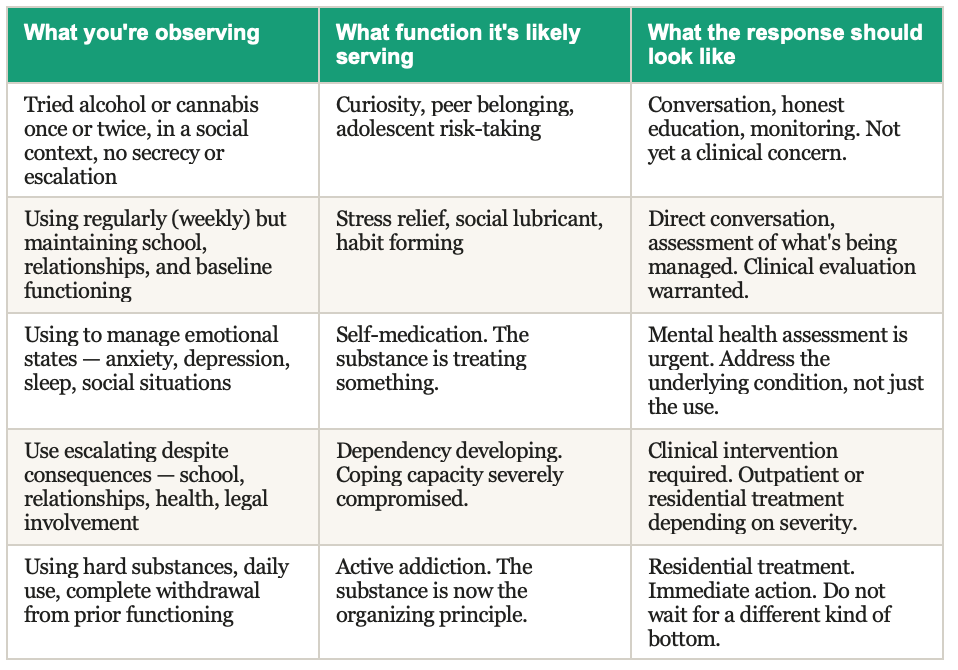
Adolescent substance use exists on a wide spectrum — from genuine experimentation with no clinical significance to active addiction requiring immediate residential treatment. Most parents, when they discover use, don't know where on that spectrum their child falls. And in the absence of that knowledge, fear tends to fill the gap.
The reframe I offer families is this: before asking "how do I stop this," ask "what is this doing for my child?"
This isn't a soft question. It's the most clinically important one. Substance use in adolescents is almost always functional. It's doing something for the person using it. Understanding what that something is changes everything about the appropriate response.
A teenager who tried cannabis twice at a party because their friends were doing it and they wanted to belong is in a fundamentally different situation from a teenager who is using every day to quiet an anxiety disorder that has never been diagnosed or treated. Both situations involve substance use. They require completely different responses.
Getting this assessment right, understanding the function before reaching for the solution, is the single most important step in responding effectively.
What teen substance use is usually treating
In the vast majority of cases I've worked with, adolescent substance use is a form of self-medication. The teenager has found something that temporarily relieves an experience they find intolerable, and they've learned to reach for it when that experience arises.
The most common underlying conditions I see:
Anxiety
Anxiety is the most prevalent underlying factor in adolescent substance use, and it's particularly common in high-achieving, high-pressure environments where asking for help feels like weakness. Cannabis, in particular, is frequently used to quiet an anxious nervous system. Alcohol is used to manage social anxiety in settings where belonging feels essential.
The cruel paradox is that both substances, over time, worsen the underlying anxiety. The short-term relief reinforces the behavior. The long-term effect deepens the problem. A teenager who starts using to manage anxiety often ends up more anxious, more dependent, and less equipped to manage the original condition than when they started.
Depression
Depression in adolescents often doesn't look like sadness, it looks like flatness, irritability, withdrawal, and a loss of interest in things that used to matter. Substances offer a temporary alteration of that internal landscape: a brief period of feeling something, or feeling nothing, that is preferable to the persistent gray of depression.
Stimulants are sometimes used by depressed teenagers to feel energy and motivation they can't access otherwise. Cannabis is used to disconnect from the weight of a depressive state. Alcohol is used to temporarily numb the flatness or to access an emotional range that depression has compressed.
Trauma
Unprocessed trauma (including experiences that don't look like what most people picture when they hear the word) frequently underlies adolescent substance use. Social humiliation, family instability, loss, chronic stress, bullying: these leave internal marks that teenagers often don't have language for, and that the clinical system often doesn't identify because the teenager has learned to manage the surface presentation.
Substances, for teenagers carrying unprocessed trauma, offer regulation of a nervous system that is chronically dysregulated. The relief is real and immediate. The cost is invisible until it isn't.
Undiagnosed ADHD or learning differences
This is one of the most consistently underrecognized patterns in adolescent substance use. A teenager with undiagnosed ADHD, particularly one who is bright enough to have compensated academically for years, often finds that cannabis produces a kind of focused calm they've never been able to access naturally. Stimulants are used, sometimes without any medical oversight, to manage attention and academic performance.
When a teenager tells you that a substance "helps them focus" or "makes them feel normal," that is not rationalization. That is clinical information about an underlying condition that hasn't been identified or treated, and it deserves a clinical response, not just a behavioral one.
Social pain
Adolescence is a period of intense social formation; of figuring out who you are in relation to others, of finding the peer context where you feel you belong. For teenagers who struggle with this, who feel outside the social mainstream, who are lonely, who are trying to fit somewhere they don't quite fit, substances often provide social currency and temporary belonging.
This is the function that is most often dismissed by parents as "peer pressure", as though the solution is simply to choose better friends. But the social pain is real, and without addressing it, a teenager who stops using in one peer context will often find a different context where use is normalized and the belonging it provides is available again.
The critical variable at every level is function. The question is not just how much or how often, but what role the substance is playing in your child's life, and what would need to be in place for them to manage without it.
What not to do. The responses that make things harder
The first responses most parents reach for when they discover substance use tend to be the ones that close the conversation rather than open it. I want to name them directly, because they come from love, and they still tend to make things worse.
Reacting with an immediate consequence
Grounding, removing privileges, confiscating phones. These responses feel like action. They communicate that you're taking this seriously. And they often produce, in the short term, exactly the opposite of what you need: a teenager who becomes more secretive, more skilled at hiding, and less likely to come to you when things escalate.
This doesn't mean consequences have no place. It means consequences divorced from understanding rarely produce the change families are hoping for, and that the conversation has to come first.
Minimizing it
"All teenagers try things." "It's just a phase." "At least it's not something worse."
These responses come from a desire to avoid overreacting. Sometimes they're accurate, sometimes it really is experimentation with no clinical significance. But the only way to know that is to investigate, not to assume. And a teenager who senses that their parents are minimizing something they're struggling with stops communicating about it.
Making it only about the substance
"We need to talk about the drugs." Conversations that begin this way almost always end with the teenager shutting down, because the substance is the symptom, and teenagers, however inarticulate they may be about what they're managing, know on some level that the conversation is missing the point.
The conversation that needs to happen is about what's going on underneath. That is a harder conversation to have. It requires curiosity instead of confrontation. It requires listening for what isn't being said as much as what is. And it almost always produces more information and more genuine engagement than leading with the behavior.
Waiting for it to get worse before acting
This is the most common mistake I see, and the costliest. Families wait because they don't want to overreact. They wait because the teenager seems functional. They wait because they hope it will resolve on its own.
Substance use in adolescents rarely resolves on its own once it has become functional. Once it is doing something for the teenager that they don't have another way to manage. What resolves on its own is genuine experimentation: use that is truly social, truly infrequent, truly without function. What grows without intervention is use that is managing something.
The earlier the underlying condition is identified and treated, the more options exist and the less entrenched the pattern becomes. Waiting is always more expensive than acting, in every sense of that word.
What the conversation should actually look like
The first conversation (the one that happens after you've discovered the use) is one of the most important conversations you will have with your teenager about this. Here is the approach I recommend:
1. Create the conditions for honesty before you speak
Choose a time when neither you nor your teenager is in a heightened emotional state. Not immediately after discovery, if you can help it. Not when you're late for something else. Not in the car, where they're trapped. Somewhere neutral, with enough time.
And before you speak, do something genuinely difficult: set aside what you want to say and commit to listening first.
2. Lead with curiosity, not accusation
"I found out that you've been using [substance]. I'm not here to punish you right now. I want to understand what's going on for you."
This will feel uncomfortable, because it isn't the natural first response, and because there's a real possibility your teenager won't believe you mean it. Do it anyway. The teenagers I've seen have real conversations with their parents about substance use are almost always the ones whose parents led with a genuine question rather than a predetermined conclusion.
3. Ask about what it does for them
"Does it help you relax? Does it help you sleep? Does it help you feel less anxious in social situations?" These questions (asked without judgment) give the teenager language for something they may not have articulated even to themselves. And the answers give you clinical information that shapes everything else.
4. Be honest about your fears without making them the center
"I'm scared about this. I want to be honest with you about that. And I also want to understand what's happening for you before we figure out together what to do next."
Teenagers respect honesty. They can tell when you're performing calm you don't feel. Acknowledging your fear, while making clear that it won't determine the entire conversation, builds more trust than pretending the fear isn't there.
5. Don't end the conversation with a conclusion
The first conversation is not the conversation where everything gets resolved. Its purpose is to open a channel, not to close a problem. End it with something that leaves the door open: "I'm glad we talked about this. I want to keep talking about it. And I want us to figure out together what kind of support might actually help."
When professional assessment is needed, and what kind
Every situation of adolescent substance use warrants some form of professional assessment. The question is what level of assessment is appropriate, and what it should focus on.
Start with a mental health evaluation
Regardless of the level or type of use, the first clinical step is a mental health evaluation by a professional who works with adolescents and who understands the relationship between substance use and underlying conditions. This evaluation should assess not just the use itself but the functional landscape around it: mood, anxiety, trauma history, attention and learning profile, social functioning.
The goal is to identify what the substance is treating, so that treatment can address the underlying condition rather than just the behavior.
Don't lead with an addiction specialist if the picture is unclear
Sending a teenager who has been using cannabis for three months to an addiction specialist before conducting a mental health assessment can pathologize a situation that is more accurately understood as undertreated anxiety or depression. The framing matters, and starting with the wrong frame can make a teenager more resistant to the help they actually need.
Start with mental health. Let the assessment guide the next step.
When residential treatment is warranted
There are situations where the level of use, the underlying clinical picture, or the degree of functional impairment warrants residential treatment. These include:
• Daily use that is significantly impairing functioning (academic, social, or family)
• Use of substances with high overdose or dependency risk (opioids, benzodiazepines, methamphetamine)
• A mental health presentation that is severe enough to require intensive support alongside substance treatment
• Multiple failed outpatient attempts that have not produced stable change
• A home environment that is not able to support the level of structure the teenager needs
Residential programs for adolescent substance use vary enormously in quality, clinical approach, and philosophy. Choosing the right one requires the same careful vetting we apply to any placement - visiting the program, understanding the clinical model, assessing the culture, and matching the program to the specific clinical picture of the teenager.
A program that is right for a teenager with co-occurring depression and cannabis dependence is not necessarily right for a teenager with trauma and alcohol use disorder. The specificity of the match matters as much here as it does in educational placement.
A note on shame (yours and theirs)
I want to address something that doesn't get said enough in these conversations.
Parents of teenagers who are using substances carry an enormous amount of shame. The fear that you caused this. That you missed something. That you're being judged by the other parents, the school, your own family. That somehow your child's struggle reflects something fundamental about your competence as a parent.
This shame is almost never warranted, and it is always in the way. It makes parents defensive when they need to be open. It makes them minimizing when they need to be honest. It makes them reactive when they need to be curious.
Your teenager is carrying shame too. The shame of being someone who uses, of having something that feels out of control, of not being able to manage what their peers seem to manage without difficulty. That shame is one of the primary reasons they didn't tell you. And it is one of the primary reasons that conversations leading with accusation or consequence tend to produce silence rather than honesty.
Both of you deserve a space where the shame is set aside, where the question is not "what went wrong" but "what is actually happening, and what does this child need." That is the conversation that produces real change.
Your teenager's substance use is not a verdict on you as a parent. It is information about your child. And information, handled with clarity and care, is the beginning of something better, not the end of something good.
What we do at Liston Education in these situations
Adolescent substance use sits at the intersection of mental health and education in a way that defines exactly what Liston Education Group was built to navigate.
We don't just place teenagers in programs. We help families understand what's actually driving the situation, through our own assessment and through coordination with the clinical team, and identify the level and type of support that matches the real clinical picture.
We know the landscape of programs: which ones have strong clinical models for co-occurring mental health and substance use, which ones are strong on the substance side but thin on the underlying conditions, which ones are genuinely therapeutic and which ones are primarily behavioral. We've visited them. We track outcomes. We know the difference.
And we stay involved after placement, because the transition home from a substance use program is one of the highest-risk periods in the entire process, and because the families that do best in that transition are the ones who have someone in their corner throughout it.
If you are navigating this situation right now, whether you discovered something recently or have been watching it escalate for longer than you want to admit, we would like to help. Not with judgment. With clarity, and with the kind of support that addresses what's actually happening.
Navigating adolescent substance use?
Liston Education Group works with families navigating the intersection of adolescent mental health and substance use, from initial assessment through program placement, long-term case management, and family coaching. We help families understand what's actually driving the situation and identify the right level of clinical support.
We work nationally, in person and remotely. We vet every program we recommend personally, because the match between your child's clinical picture and the program's model is everything.
Let’s have a conversation about your family and where things stand. Reach out when you're ready.
About the author
Jodi Liston is the founder of Liston Education Group, a concierge educational and therapeutic consulting firm. She has spent more than 30 years helping families navigate complex academic, emotional, and behavioral challenges — including adolescent substance use, therapeutic program placement, school placement, long-term case management, and special education advocacy. She came to this work in part through her own experience as a parent navigating these systems, and that experience shapes every family she works with.